Introduction
Sensorineural hearing loss is common in patients with chronic kidney disease (CKD), occurring in 29% of children with end-stage renal disease and in 47% after renal transplantation 1. CKD leads to immunosuppression, which has been reported to be associated with poor wound healing and/or infection. These issues are leading causes of morbidity in patients receiving solid organ transplantation 2. For cochlear implantation, the common cause of morbidity is wound complication and meningitis. Due to these risks, cochlear implantation is rarely undertaken in a patient who underwent a renal transplant.
Case
A 12 year old male was diagnosed at age 2.5 years to have a posterior urethral valve leading to reflux nephropathy. This progressed to chronic renal failure, and subsequently end-stage renal disease (ESRD). He underwent fulguration of the posterior urethral valve , and seven years later he developed renal infection for which he received intravenous antibiotics. Within a week, he developed bilateral tinnitus and a sensorineural hearing loss, which gradually worsened. He was fitted with bilateral behind-the-ear hearing aids at that time. The child underwent a renal transplant in 2008 at the age of 10 years and is currently on immunosuppressive drugs (Cyclosporin, Prednisolone, Mycophenolic acid and Lercanidipine Hydrochloride) since then. Deterioration of function in the grafted kidney occurred and he underwent a percutaneous nephrostomy.
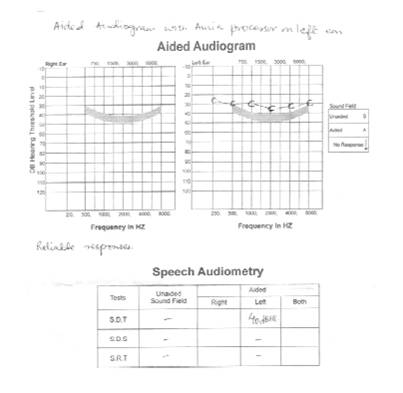
Pure tone audiogram (PTA) showed profound hearing loss (pure tone average of 100dB) in the right ear, and a severe to profound hearing loss (pure tone average of 85 dB) in the left ear, with absent otoacoustic emissions bilaterally. High resolution CT scan (computerized tomography) and MRI (Magnetic Resonance Imaging) of inner ear and brain did not reveal any abnormalities. After consultation with the child’s parents, audiologist, nephrologist, and ENT specialist, the child received a cochlear implant at the age of 12 years in his left ear (i.e. 2 years after his renal transplant). The child received meningococcal, pneumococcal and hemophilus influenza vaccination 10 days prior to surgery. Intra operatively, the child received Injection Co-amoxiclav, which was continued perorally in form of suspension for 10 days post-operatively. The child’s immunosuppressive drug regime was not changed during, or after, implant surgery. At present, the cochlear implant aided audiogram shows hearing within speech banana curve (figure 1), speech discrimination score (SDS) is 80 % six sound tests achievable from 12 feet, a CAP ( Categories of Auditory performance) score of 9 out of 12 and a MAIS( Meaningful Auditory Integration Score) of 35/40.

Figure 1. Cochlear implant aided audiogram showing hearing thresholds above speech banana curve in left ear
Discussion
Sensorineural hearing loss is common in children with CKD and persists after kidney transplantation 2, 3. Periodic audiological assessment and strict monitoring of ototoxic therapy should be carried out. A significant correlation has been found between hearing loss and the administration of ototoxic drugs like aminoglycosides and furosemide, and in patients on dialysis with changes in fluid and electrolyte composition of the endolymph. Expected speech discrimination score for postlingually deafened adults or children after cochlear implantation range from 70% to 80% for open-set sentence tests, and 35% to 45% for open-set word tests 2. The performance of our patient falls in this range.
Children after transplantation have an increased risk of infections due to immunosuppressive therapy 4. Infection and delayed wound healing are the leading causes of morbidity and mortality among organ transplant recipients. These are also important issues in cochlear implant surgery. Our patient suffered no complications peri- or postoperatively, and is clinically well 1 year after cochlear implantation.
Bacterial infections are the most common and are mainly related to gram-negative bacteria. The high prevalence of Pseudomonas Aeruginosa is consistent with nosocomial infection and occurs mainly in first month after surgery. Between 1 and 6 months, there is an increased risk of opportunistic infections and after 6 months, most infections are commonly acquired. Additionally, there is an elevated risk of infection related to invasive devices 5. Commonly used drugs after kidney transplant are Cyclosporin, Prednisolone, Myfortic (Mycophenolic acid), and Lotensyl (Lercanidipine hydrochloride). Liver transplants carry higher infection risks due to more common use of cyclosporine, which inhibits cytotoxic T cells 6. The introduction of Mycophenolate Mofetil and Sacrolimus did not result in a significant increase in transplant wound-healing complications 7. The anti inflammatory effect of immunosuppressive drugs peaks between 1 and 6 months, this should be considered before undertaking a cochlear implant surgery 2. Severe intracranial infections can occur due to the insertion of such a device, so cochlear implants have not been generally described in children following kidney transplantation. In our case we showed that with antibiotic prophylaxis and an unchanged immunosuppressive drug regime, a cochlear implant can be inserted without complications. Care should be taken not to miss any immunosuppressive medication, and immunization prior to transplantation against pneumococci and meningococci should be done. The standard preoperative work up and close communication with the renal transplant team is advisable for safe and effective cochlear implantation after renal transplant.
Abbreviation
CKD: Chronic Kidney Disease
ESRD: End Stage Renal Disease
MRI: Magnetic Resonance Imaging
CT Scan: Computed Tomographic Scan
SDS: Speech Discrimination Score
CAP: Categories of Auditory Performance
MAIS: Meaningful auditory integration Score
PTA: Pure Tone Audiogram
References
1. Mancini ML, Dello Strologo L, Bianchi PM,Tieri, Rizzoni G. Sensorineural hearing loss in patients reaching chronic renal failure in childhood. Pediatr Nephrol 1996; 10(1): 38-40.
Publisher – Google Scholar
2. Patterson MD, Telischi FF, Connell SS, Ulubil AS, Hodges VA, Eshraghi AA, Balkany JT. Cochlear Implantation in Organ Transplantation. Laryngoscope 2008; 118: 116-19.
Publisher – Google Scholar
3. Gatland D, Tucker B, Chalstrey S, Keene M, Baker L. Hearing loss in chronic renal failure-hearing threshold changes following hemodialysis.J R soc Med 1991;84: 587-589.
Google Scholar
4. Zimmerhacki LB, Wiesmayr S, Kirste G, Jungraithmayr T. Mycophenolate mofetil (cellcept) in pediatric renal transplantation. Transplant Proc 2006; 38: 2038-40.
Publisher – Google Scholar
5. Guaraldi G, Cocchi S, Codeluppi M, et al. Outcome, incidence, and timing of infectious complications in small bowel and multivisceral transplantation patients. Transplantation 2005; 80:1742-48.
Publisher – Google Scholar
6. Tannenbaum DA, Mathews LS, Grady-Benson JC. Infection around joint replacements in patients who have a renal or liver transplantation. J Bone Joint surg Am 1997; 79:36-43.
Google Scholar
7. Fletcher SM, Zhou L, Derweesh I, Mastroianni B et al. The Impact Of Sirolimus, Mycophenolate Mofetil, Cyclosporine, Azathioprine and Steroids on wound healing in 513 Kidney-Transplant Recipients. Transplantation 2003; 76: 1729-34.
Publisher – Google Scholar