Introduction
Urinary retention is uncommon among women and often results from urethral surgeries, drugs, and psychic by Barber 1938. Fistulae causing or occurring concurrently with retention of urine is an unusual phenomena; Crichton 1954 has described only one case in English literature. Other related common complications of fistulae include stone formation, excoriative vulva dermatitis, and social stigmatization by Hancock 2009. A case of urinary retention as a complication of urethra-vaginal fistula is presented with its management.
Case Presentation
A 27-year-old Tanzanian woman, para two presented with history of failure to control passage of urine for 9 months. Problems started following prolonged and neglected labour where she ended up with stillborn of 2.6 Kg. She started laboring at home for hours then went to nearby hospital where she was able to spontaneously deliver vaginally. She reported to have had Cesarean delivery in her first pregnancy, in which there were no complications, and a healthy baby was born. She denied both history of pain related to incontinence of urine and history of fever.
Physical examination: young woman, ammoniac smell, afebrile, not jaundiced, and normal nutritional status. Vital signs were stable at the time of admission.
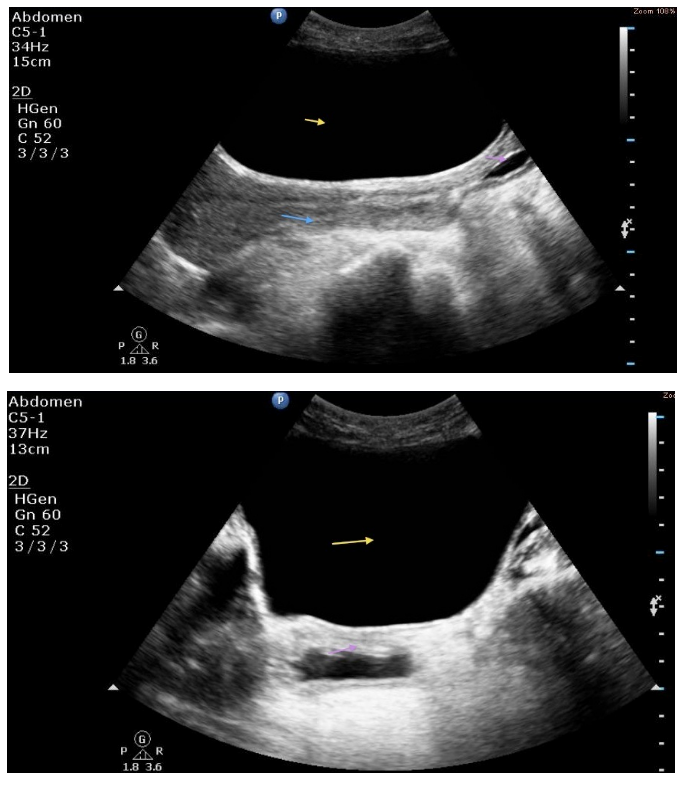
Examination of the abdomen revealed a sub-umbilical midline surgical scar with distension on suprapubic area. A soft and smooth mass was palpable on suprapubic area, with size equivalent to uterine fundus of 16 cm, notably there was only sideways mobility.
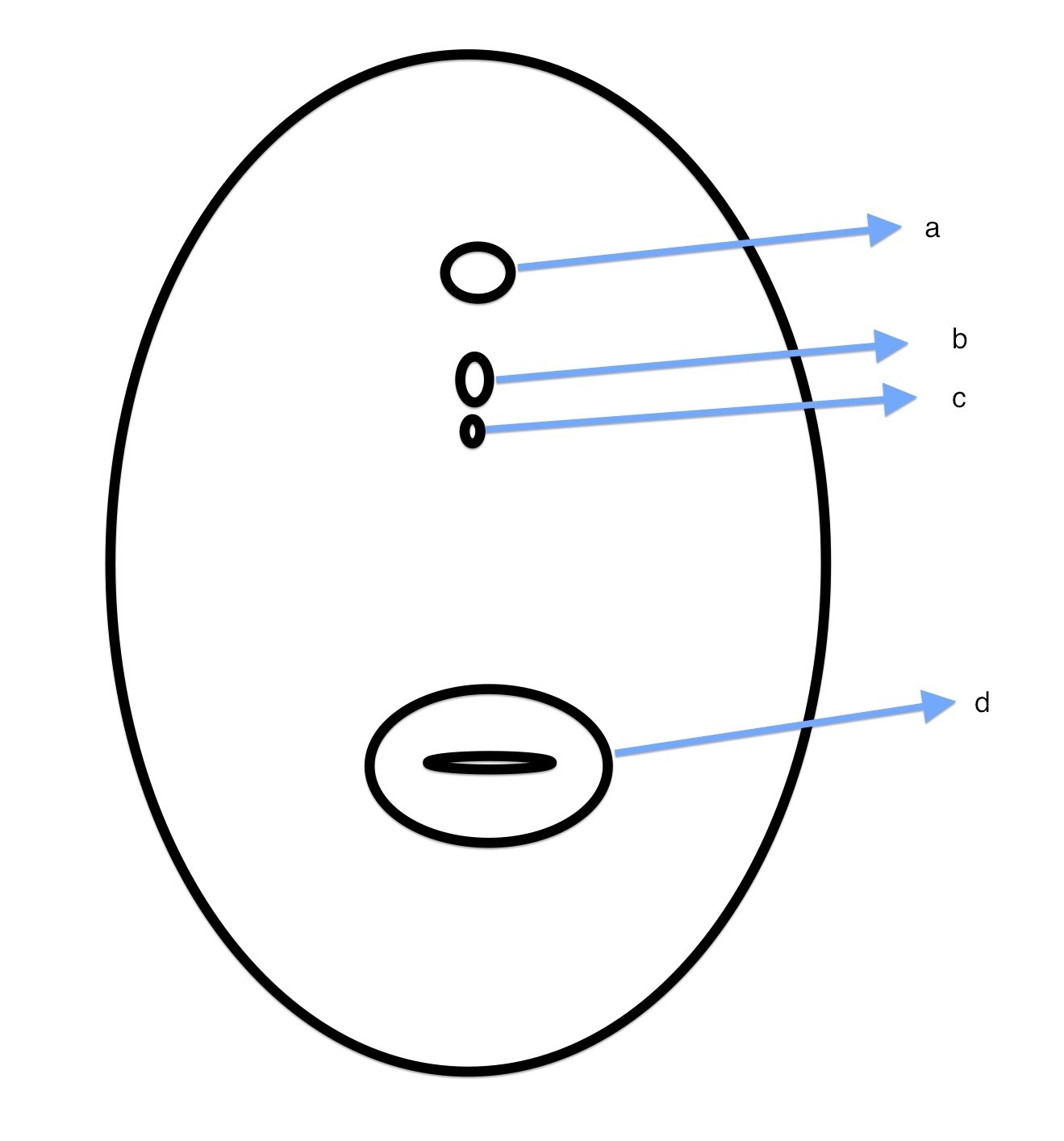
Speculum and digital examination showed a scarred defect on anterior vaginal wall about 2 cm from urethral meatus. However, the cervix and posterior vaginal wall were normal. Pool of urine accumulated in the vagina was found.
Hence, additional test for creatinine was ordered, which was found to be within normal range.
The final impression was urethro-vaginal fistula with chronic urine retention.
She was counseled and agreed to urethro-vaginal fistula repair trans-vaginally in theatre. Findings in theatre: a fistula tract identified about two centimeters from urethral meatus. Distal part of the urethra was patent, however the proximal part of it was partially obstructed causing retention of urine with minimal leakage. Metal catheter was inserted through the urethral meatus for guidance of fistula dissection and repair. Hydro-dissection was performed using a specially formulated solution (“jungle juice” consists of adrenaline, lignocaine and sterile water). Fistula margins were dissected with scalpel, then scissors to separate the urethra and bladder from the vaginal tissue. Some scarred tissues were excised. Urethral and bladder tissue was freed from tension. Repair of the urethra was commenced in a vertical direction, inverting the tissue inward using interrupted sutures (polysorb #3-0). Methylene blue solution was used to test if watertight closure was achieved. There was no leaking on dye testing; hence vagina was repaired in transverse direction using polysorb # 0. Finally, vagina was packed with gauze to control bleeding.
Postoperative Foley catheter was retained for 21 days, and there were no complications. Foley catheter was removed after 21 days, but she developed retention of urine in the second day after removal. Attempt to re-insert catheter was successful; however there was some resistance at the time of re-insertion. Urethral stenosis was suspected, so catheter was retained for 28 days more. She was completely cured after additional 28-day stay with Foley catheter.
She was discharged in good condition with instructions to attend prenatal services in subsequent pregnancy and have an elective delivery. She should wait to resume sex intercourse for 3 months.
Discussion
If encountered in men, the problem of urinary retention is more often related to gonococcal infections and prostate abnormalities by Santucci (2004). It is uncommon among women, and its management may differ depending on the cause of retention. Fistula is associated with many other complications but not urinary retention. It may be a complication following surgery involving the urethra by Santucci (2004).
Management of urinary retention goes hand in hand with repair of fistulae. Delay in repair causes prolonged overstretching of the bladder from chronic urine retention usually results in other complications such as bladder atony, urinary tract infections, and renal failure by Anger (2010).
Although the most common treatment of urethral stenosis or stricture is urethrotomy or dilation, we opted for prolonged re-catheterization in this situation as it allows the repaired defect to continue healing. Disadvantages of prolonged catheter include risk of urinary tract infections and patient’s discomfort by Barber (1938).
Like any fistulae cases that involve the urethra, detrusor instability and stress incontinence are the likely complications. Thus, vertical repair of the urethral defect was favored, which does not impair the length of the urethra as reported by Hancock (2009).
Generally all patients who have undergone fistula repair surgery are advised to have elective delivery. The patient has a higher chance of having a safe elective abdominal than a safe vaginal delivery as proposed by Hancock (2009). I believe that one needs to be experienced and know what type of patient may benefit from vaginal attempt after successful fistulae repair.
Due to the problem of accessing health facilities, the Tanzania Ministry of Health has introduced “maternal waiting home”. This approach seems to solve the problem of far distance from a healthy facility (UNFPA). As for this patient, decision-making at the family level will continue to be a challenge. She had the audacity to attempt delivery at home with one previous cesarean scar. Another strategy must be invented to change health-seeking behavior.
Obstetric fistulae complicated with urinary retention can occur, and surgical repair does in fact seem to have a good outcome if prolonged catheterization is taken into consideration.
References
Anger et al.: (2010) The morbidity of urethral stricture disease among male Medicare beneficiaries. BMC Urology. 10:3.
Publisher – Google Scholar
Barber S.H. (1938) Postoperative retention of urine and its treatment. Irish Journal of Medical Science. 13, 2, 68-87.
Publisher – Google Scholar
Crichton D, (1954) Vesico-vaginal Fistula Associated with Retention of Urine. British Medical Journal. 1(5128): 1020.
Publisher
Hancock B, Browning A. (2009) Obstetric fistulae: cause and nature; the obstetric complex; classification. Practical obstetric fistula surgery. Royal Society of Medicine press ltd .1: 1-4
Santucci R, Joyce G, Wise M: (2004) Male urethral stricture disease. Urologic Diseases in America US Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. Washington, DC: US Government Publishing Office, NIH Publication No. 04-5512 Litwin MS, Saigal CS533-551 http://www.uda.niddk.nih.gov.