In spite of the legalization of abortions under the ‘MTP Act’ in India, it is not unusual to find them being performed by untrained or less trained persons, at times leading to serious maternal complications. ‘Anal menstruation’ as a result of sigmoidouterine fistula originating from the anterior surface of the uterus has hitherto been unheard of.
A colouterine fistula was first reported by Lejemtel in 1909 with three main etiologies under consideration: uterine trauma, an abscess rupturing into the bowel and the uterus, and uterine or sigmoid carcinoma. Mandato et al (2012) mention that so far, about twenty such cases have been reported in the literature.
Woods et al (1988) found that out of various possible unnatural connections between the genitourinary tract and the bowel, the colovesical fistula was the most common, followed by colovaginal fistula. The rarity of sigmoidouterine fistulas is probably explained by the fact that the uterus is a thick muscular organ, which poses obstacles for invasion for both benign and malignant disease. Colcock and Stahman (1972) suggested that such a fistula could result from the spontaneous rupture of gravid uterus, obstetric traumatic procedure such as curettage, uterine or colonic cancer, radiotherapy or an inflammatory process like diverticulitis and periappendicial abscess. Although the exact mechanism of development of sigmoidouterine fistula in our case is not very clear, it may be postulated that the inflammatory adherence of the bowel wall (rendered susceptible due to tuberculosis) to the uterus (which perforated during medical termination in unsafe hands) could have resulted in subsequent fistula formation.
Sigmoidouterine fistula may result into chronic vaginal discharge which may be purulent, hemorrhagic or fecal in nature. However, our patient presented with a very unusual symptom of ‘anal menstruation’ in the absence of periodical normal menses. Normally, one would have thought of hemorrhoids, large bowel pathology, and recto-sigmoid endometriosis etc. as a possible cause of such bleeding but the absence of normal menses altogether forced us to think of reverse flow of menstrual blood through the fistulous tract in the presence of cervical stenosis responsible for ‘anal menstruation’. Cervical stenosis might have resulted from the trauma and infection associated with dilatation and curettage performed by an inexperienced person. The retroverted gravid uterus might have predisposed to injury to the anterior wall of the uterus while performing dilatation and curettage by an inexperienced hand. The reason of one way flow from the uterus to sigmoid colon and not the other way was perhaps due to thicker fecal contents of sigmoid colon as compared to menstrual blood and the distal obstruction in the uterus. This assumption gained strength from the fact that the patient started having natural menstruation after the cervical dilatation and excision of fistulous tract. Reverse flow of menstrual blood in adequate amount through the anus prevented the development of hematometra, hematosalpinx, and endometriosis. The absence of purulent or fecal discharge per vaginum could also result from cervical stenosis and tapering tract at the uterine end.
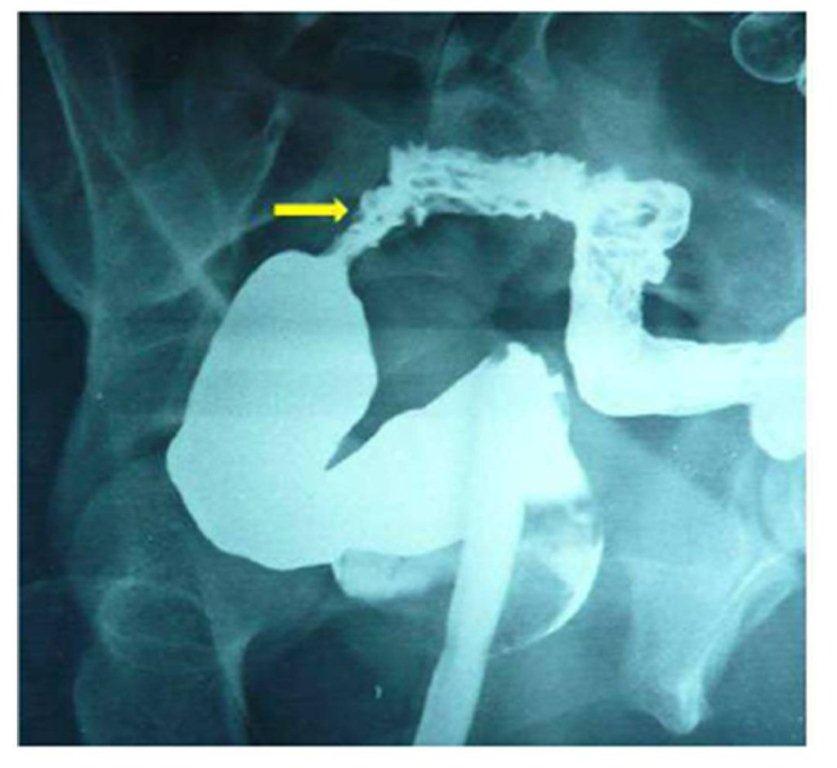
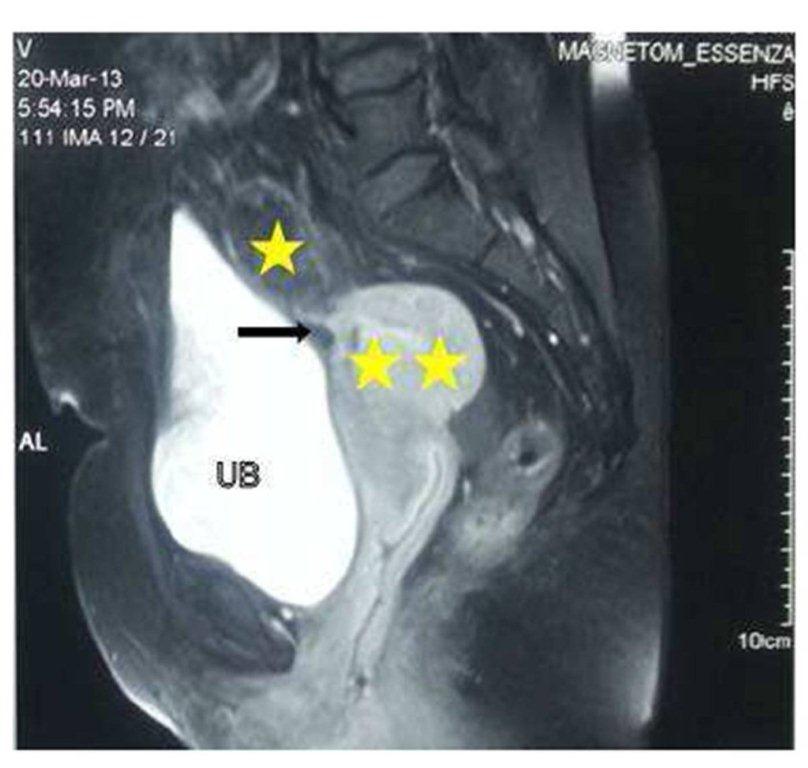
Many imaging modalities have been suggested and tried for establishing the diagnosis of sigmoidouterine fistula. Whereas CT scan can establish the diagnosis of diverticular disease, its role in demonstrating the fistula may be limited. Moreover, it is associated with a high dose of radiation. Beattie et al (2005) are of the opinion that multidetector computed tomography (MDCT) provides better visualisation of fistula, but it is associated with still greater radiation. Kassab et al (2008) have found MRI to be a more versatile, sophisticated and accurate diagnostic tool in showing the fistula. Huetter et al (1992) suggested that Charcoal Challenge Test could prove to be a non-invasive useful modality for the diagnosis of such an entity, but was not done by us as it cannot identify the exact site of the fistula and the tract. Sonohysterography is another modality for the diagnosis of such entity but needs costly contrast media.
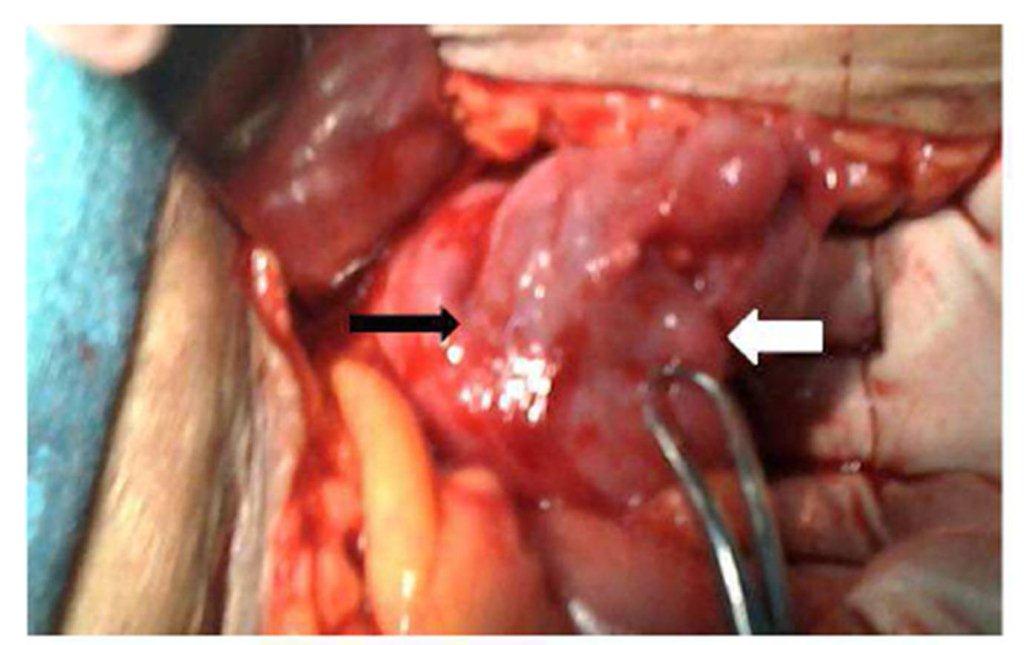
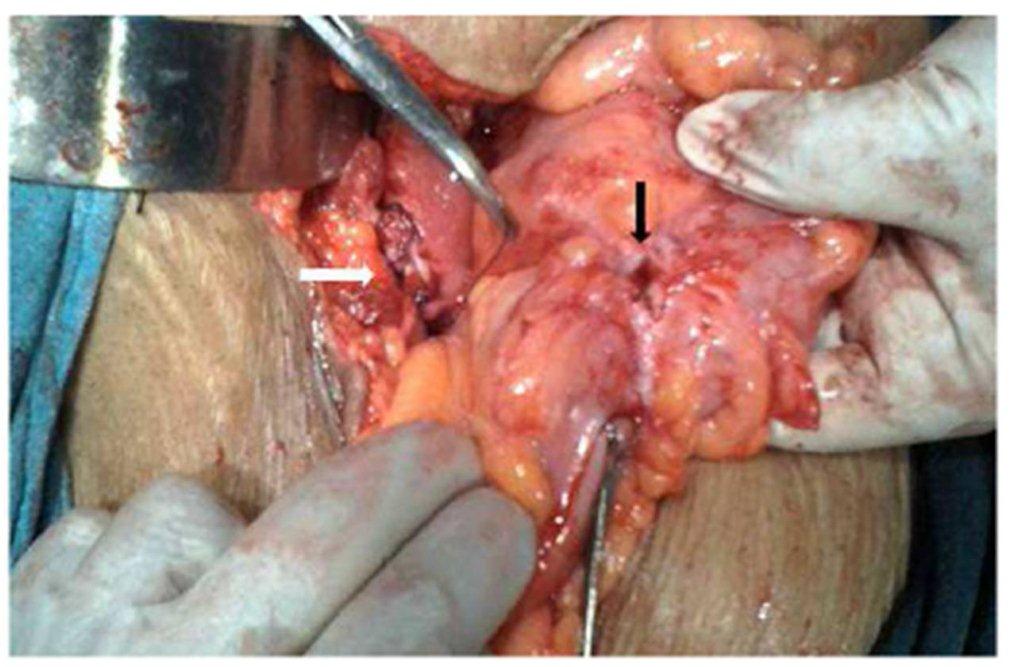
Surgical treatment was a one-stage operation in our patient without sacrifice of the uterus or two stage colonic repair. En bloc, resection of the uterus and sigmoid colon is preferred if malignancy cannot be excluded. Hysterectomy may also be mandatory to extirpate a nidus of acute infection particularly in older woman who has completed her family. Severe local inflammation or obstruction of the bowel may necessitate a two-stage procedure involving resection and end colostomy, followed by re-anastomosis at a later date.
Precis
Anal menstruation as a result of sigmoidouterine fistula may complicate unsafe abortion and requires high degree of suspicion and planned investigations for proper management.
Source of the work
It was the patient admitted in the Obstetrics and Gynecology ward of Sir Sunderlal Hospital attached to the Institute of Medical Sciences, Banaras Hindu University, VARANASI.
No financial support was received for this report. There is no conflict of interest.
References
1. Beattie, G.C., Nelson, M. and McMillen , I.M.(2005) “McMurray AH. Colouterine fistula mimicking pyometrium–diagnosis established with multi-detector computed tomography.” Ulster Med J, 74(1), 51-53.
Google Scholar
2. Colcock, B.P. and Stahman, F.D. (1972) “Fistula complicating diverticular disease of the sigmoid colon.” Ann Surg, 175, 838-846.
Publisher – Google Scholar
3. Huetter, P.C., Finkler, N.J. and Welch, W.R.(1992)” Colouterine fistula complicating diverticulitis: charcoal challenge test aids in diagnosis.” Obstet Gynecol, 80(3 pt 2), 550-552.
Google Scholar
4. Kassab, A., El-Bialy,G. and Hashesh, H.(2008) “Magnetic resonance imaging and hysteroscopy to diagnose colo-uterine fistula: a rare complication of diverticulitis.” J Obstet Gynecol Res, 34, 117-120
Publisher – Google Scholar
5. Mandato,V.D.,Abrate,M. and Sandona, F.(2012) “Colouterine fistula complicating diverticulitis diagnosed at hysteroscopy: case report.” J Minim Invasive Gynecol, 19(1),118-121
Publisher – Google Scholar
6. Vilallonga, R., Baena, J.A. and Fort, J.M. (2009) “Colouterine fistula complicating diverticulitis in elderly women.” Int J Colorectal Dis, 24(5), 599-600.
Publisher – Google Scholar
7. WHO (2011), Unsafe Abortion: Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality in 2008, sixth Ed.
Google Scholar
8. Woods,R.J., Lavery,I.C. and Fazio, V.W.(1988) “Internal fistulas in diverticular disease”. Dis. Colon Rectum, 31,591-596
Publisher – Google Scholar