Volume 2014 (2014),
Article ID 396352,
Research in Endocrinology,
6 pages,
DOI: 10.5171/2014.396352
Received date: 11 November 2013; Accepted date: 25 March 2014; Published date: 29 April 2014
Academic Editor: Athina Pyrpasopoulou
Cite this Article as:
Hans-Jacob Haga, Alicia Martin Moreno, Dorte Terp Andersen and Elisabeth Peen (2014), "Serum-Prolactin and the Association to Disease Activity in Patients with Rheumatoid Arthritis," Research in Endocrinology, Vol. 2014 (2014), Article ID 396352, DOI: 10.5171/2014.396352
The objective of this article is to analyze the serum level of Prolactin (s-PRL) in 307 treated patients with Rheumatoid Arthritis (RA), and its association to disease activity, demographics, serological and clinical variables. The hypothesis to be tested: s-PRL correlates to disease activity in RA. Serum concentration of the hormone Prolactin (s-PRL) was determined in 307 treated patients with (RA) in a cross-sectional study design. The patients were characterized by demographic, serological and clinical variables, in addition to assessment of disease activity by DAS28 (3w-CRP) score. Prolactin was analyzed by a double sandwich immune analysis. Among the 307 RA-patients examined, only 4 patients had high s- PRL defined as females > 637 mIU/L, and males > 456 mIU/L. These 4 patients all had low disease activity score (DAS 28 score < 2, 0). There was no correlation of s-PRL to DAS28 score (r= – 0, 08, p=0.21), and no correlation of s-PRL to the number of swollen or tender joints, pain, CRP, Rheumatoid factor or anti-CCP. We demonstrated that 4 out of 307 RA patients had high level of s-PRL, all of them with low disease activity score. No correlation of s-PRL to disease activity DAS 28 score was demonstrated. We therefore question the hypothesis that PRL may play a role in disease severity and the development of rheumatoid arthritis.
The hormone prolactin (PRL) is secreted from the pituitary gland and other organs and cells, particularly lymphocytes. The hormone has immunstimulatory effects and may promote autoimmunity, mainly by inhibition of negative selection of autoreactive B lymphocytes as described by Orbach H et. al .(2007) and Chuang E et. al. (2007). PRL is a cytokine, and enhances the the proliferative response to specific antigens and mitogens as demonstrated by Athreya B.H et. al. (1993). Hyperprolactinemia (HPRL) is observed in autoimmune diseases like Systemic Lupus Erythematosus (SLE), Rheumatoid Arthritis (RA), psoriasis, celiac disease, Sjögren’s syndrome , Hashimoto’s thyrioiditis and Systemic Sclerosis as reviewed by Shelly S et. al. (2012).
It has been suggested by Chikanza I.C (1996) that excessive PRL secretion may be of pathogenic importance in RA. Increased level of s-PRL has been reported in patients suffering from RA demonstrated Zoli A et. al. (2002), Ram S et. al. (2004), Seriolo B et. al. (2002), and Fojtikova M et. al. (2010), and there has been reported a correlation between disease activity and the level of PRL in synovial fluid, as well as a correlation of s-PRL to the total Larsen radiographic score Fojtikova M et.al. (2010). However, the data demonstrating an association between s-PRL level and disease activity are inconsistent as demonstrated by Gutierrez M.A et. al. (1999), Berczi I et. al. (1987), and Nagy E et. al . (1991). None of the present studies, however, have correlated s-PRL to modern disease activity scores such as DAS 28 commonly used in daily clinical practice and in research.
In the present study we analyzed the serum level of prolactin in 307 treated patients with RA, and its correlation to disease activity, laboratory parameters and demographic data. The hypothesis to be tested is: s-PRL correlates to disease activity in patients with RA. Methods
At the outpatient clinic at Sydvestjysk sygehus in Esbjerg, about 700 patients with RA were treated and regularly monitored. Among these we included 307 patients in the period from september 2005 to october 2006 after they had given a written informed conscent. The patients were diagnosed with RA according to the ACR-1988 criteria as defined by Arnett F.C et. al. (1988), and an additional inclusion criteria was age > 18 years.
Controls were not included as the main aim of our study was to study correlation between serum prolactin and disease activity of RA, and not a study of the serum level of prolactin in RA patients versus controls.
Four physicians participated in the study, and the patients were evaluated at their regular visits by the disease activity score DAS 28, (3w- CRP) , pain vas score range 0-100, and ordinary blood samples. Blood samples were also analyzed for the presence of Rheumatoid Factor by an ELISA technique, and for anti-CCP by the ELISA IgG system on the UniCap 100 from Pharmacia Diagnostics. Blood samples for analysis were collected between 10.00 and 13.00 am., and were then stored at — 800 C.
Prolactin was analyzed by a double sandwich immune analysis using polyclonal goat antibody against PRL (ADVIA Centaur), and all samples were analyzed on the same day. The laboratory defined the normal level of s-prolactin for women to be < 637 miu/l, and for men < 456 miu/l,
Statistical Methods
Comparing groups of variables were performed using Chi-square test and one-way — ANOVA test. P-values < 0.05 were regarded as statistically significant.
Correlation analysis was performed by partial correlation analysis and Spearman rank correlations.
Results
307 patients with RA participated, 210 women (68.4 %) and 97 men (31.6 %). The mean age at examination was 62.8 years (19-87 years), and the mean time since diagnosis was 10.6 years (0-50 years). Positive rheumatoid factor (RF) was detected in 247 patients (80.5 %), and positive anti-CCP was detected in 207 patients (67. 4 %).
The mean pain VAS score was 29. 93 (0-100). Rheumatic nodules were observed in 23.4 % of the patients, and vasculitis in 1 patient.
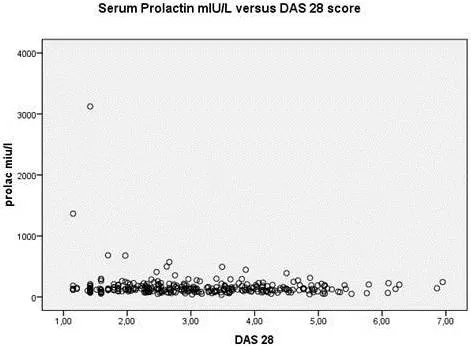
Among the 307 RA-patients examined, 303 patients had a s-PRL level within the normal range as defined < 637 and < 456 mlU/l for women and men respectively. Four patients had high serum level of PRL defined as females > 637 mIU/L, and males > 456 mIU/L. They were all females, 3 of them being anti-CCP positive, age 32-63 years, none were presently on prednisolone, and only one of them had been treated with biologics. They all had low DAS28 score at the examination, being 1.97, 1.42, 1.70 and 1.15 respectively (Figure I). The patient with the highest level of s-PRL 3122 miU/l was lactating after giving birth.
As shown in Table I, the serum level of PRL was higher in females vs. males, and in younger (< 45 years) vs. older patients. There was a non-significant trend of higher PRL serum level in short (< 1 year) vs.long disease duration, while there was no significant differences in the various groups of patients differing in serology and treatment.
There was a moderate negative non-significant correlation of s-PRL to DAS28 score (r= – 0.08, p=0.21). Serum-PRL was not significantly different in RF positive/negative, nor in anti-CCP positive/negative patients. There was no correlation of s-PRL to the number of swollen or tender joints, pain or CRP.
Discussion
It has been suggested by Chikanza I.Cet.al (1996) that excess prolactin levels may be of pathogenic importance in rheumatoid arthritis. This view is based on the demonstrated immunmodulating effect of prolactin demonstrated by Orbach H et. al. (2007), Chuang E et. al. (2007), Athreya B.H et. al. (1993), and Shelly S et. al. (2012), supported by several studies demonstrating increased serum level of prolactin in patients with rheumatoid arthritis Zoli A et. al .(2002), Ram S et. al. (2004), Seriolo B et.al. (2002), and Fojtikova M et. al. (2010). Additionally it has been reported a correlation between disease activity and the level of PRL in synovial fluid, and a correlation of s-PRL to the total Larsen radiographic score as demonstrated by Fojtikova M et. al. (2010), implicating that prolactin may play a role in disease severity and the process of joint damage.
However, the data demonstrating an association between s-PRL level and disease activity are inconsistent as demonstrated by Gutierrez M.A et. al. (1999), Berczi I et. al. (1987), and Nagy E et. al. (1991). This discrepancy may be due to the use of different tools to analyze disease activity in RA. Some of these tools have been shown not to reflect disease activity of RA, however, and has been replaced by more specific disease activity scores such as DAS 28, now in daily use in clinical practice. We are the first to correlate the disease activity score DAS 28 to the serum level of prolactin in a large population of patients.
We chose DAS 28- 3w for scoring the disease activity as it has been proposed that in established RA it is better to use the DAS index with only 3 variables, as global health or patient global assessment of disease activity can be considered mixed variables that combine the effects of the disease process and damage as suggested by Van Gestel A. M et al (1999).
In the present study 303 out of 307 RA patients had a s-PRL level within the defined normal range, while 4 patients had high serum level (hyperprolactinemi HPRL), giving a 1, 3 % prevalence of HPRL. The rate of HPRL in a healthy population is reported to be 0.4- 3% as shown by Allen S.H et. al. (1996), Biller B.M et. al. (1999), and Miyai K et. al. (1986).
It has recently been suggested by Adán N et. al. (2013), based on results from animal studies, that prolactin has a protective effect against inflammation-induced- chondrocyte apoptosis and that hyperprolactinemia has a therapeutic potential to reduce permanent joint damage and inflammation in RA. This observation is interesting in view of our observation that our patients with high levels of prolactin HPRL all had low disease activity. It also indicates that the effect of prolactin is locally in the joints and therefore may not be reflected at the serum level.
As a conclusion, we demonstrated that s-PRL did not correlate to disease activity, serology or demographic factors in 307 treated patients with rheumatoid arthritis.
We therefore question the hypothesis that PRL may play a role in disease severity and the development of rheumatoid arthritis in humans.
Table I. Differences in Serum Level of Prolactin in 307 Patients with Rheumatoid Arthritis, Comparing Various Demographic, Clinical and Serological Variables
The laboratory defined the normal level of s-prolactin for women to be < 637 miu/l, and for men < 456 miu/l,
Figure I: Scatterplot for the Serum Level of Prolactin versus DAS 28 Score in 307 Treated Patients with Rheumatoid Arthritis (RA)
The laboratory defined the normal level of s-prolactin for women to be < 637 miu/l, and for men < 456 miu/l,
Acknowledgments
We are grateful for excellent help given by the clinical and laboratory staff at the Department of Rheumatology at The Sydvestjysk sygehus, especially Dr. Yusuf Naderi, Karin Bundesen, Jytte Krause, and Pia Rasmussen.
We appreciate Kvinherrad Rheumatism Association and Stord Rheumatism Association for their funding of the project. We also thank the patients for their participation.